
Blocks away from the Coney Island Beach and Boardwalk, Zachary listens to the humming of the refrigerated trucks-turned-morgues parked outside the hospital where he works, counting the growing number of dead. Was it 16 yesterday? Or was that last week? The contours of time melt away when you’ve worked 17 consecutive 12-hour shifts, but then again, much of Zachary’s 84-hour work week is spent trafficking in uncertainties.
Like thousands of travel nurses, a type of short-term-contracted health-care worker trained to mobilize during a national crisis, he doesn’t know what will happen with any of the COVID patients he sees on a daily basis. Nor does he know what will happen to him after reusing the same N95 mask and bunny suit five days in a row.
He’s tired, but he knows at the very least that he’s helping. “I’ve never worked this many 12-hour shifts in a row or anywhere near it, but I have the skill set to be of service,” Zachary, a pseudonym, says. “I’ve learned from my uncle who’s a Navy Seal that you’ve just got to compartmentalize and keep moving forward, not letting what we see or the chaos drag you down in the process.” True to form, Zachary is nearly dogmatic about having a positive outlook. After all, when you’re walking the edge of a cliff, the last thing you want to do is look down.
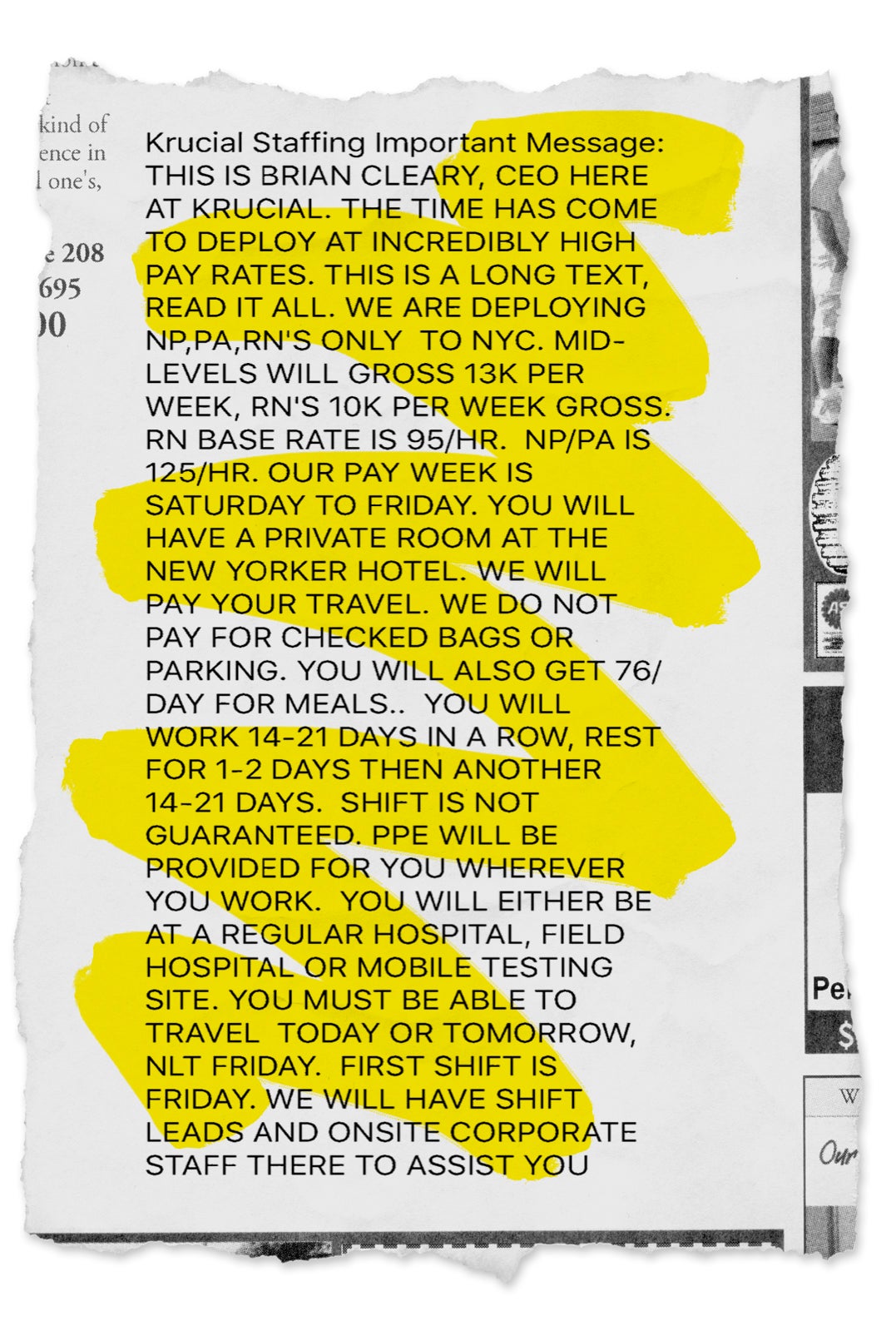
The money helps too. On average, graduate nursing students finish school about $40,000 to $55,000 in debt, the American College of Nursing reports. Zachary, who was nearly $200,000 in student debt last year, couldn’t turn down the chance to make $30,000 in just three weeks. If anything, it seemed too good to be true when robo-calls and all-caps texts from the travel nursing recruitment agency Krucial Staffing started rolling in the first week of March, reading “THE TIME HAS COME TO DEPLOY AT INCREDIBLY HIGH PAY RATES. THIS IS A LONG TEXT, READ IT ALL.”
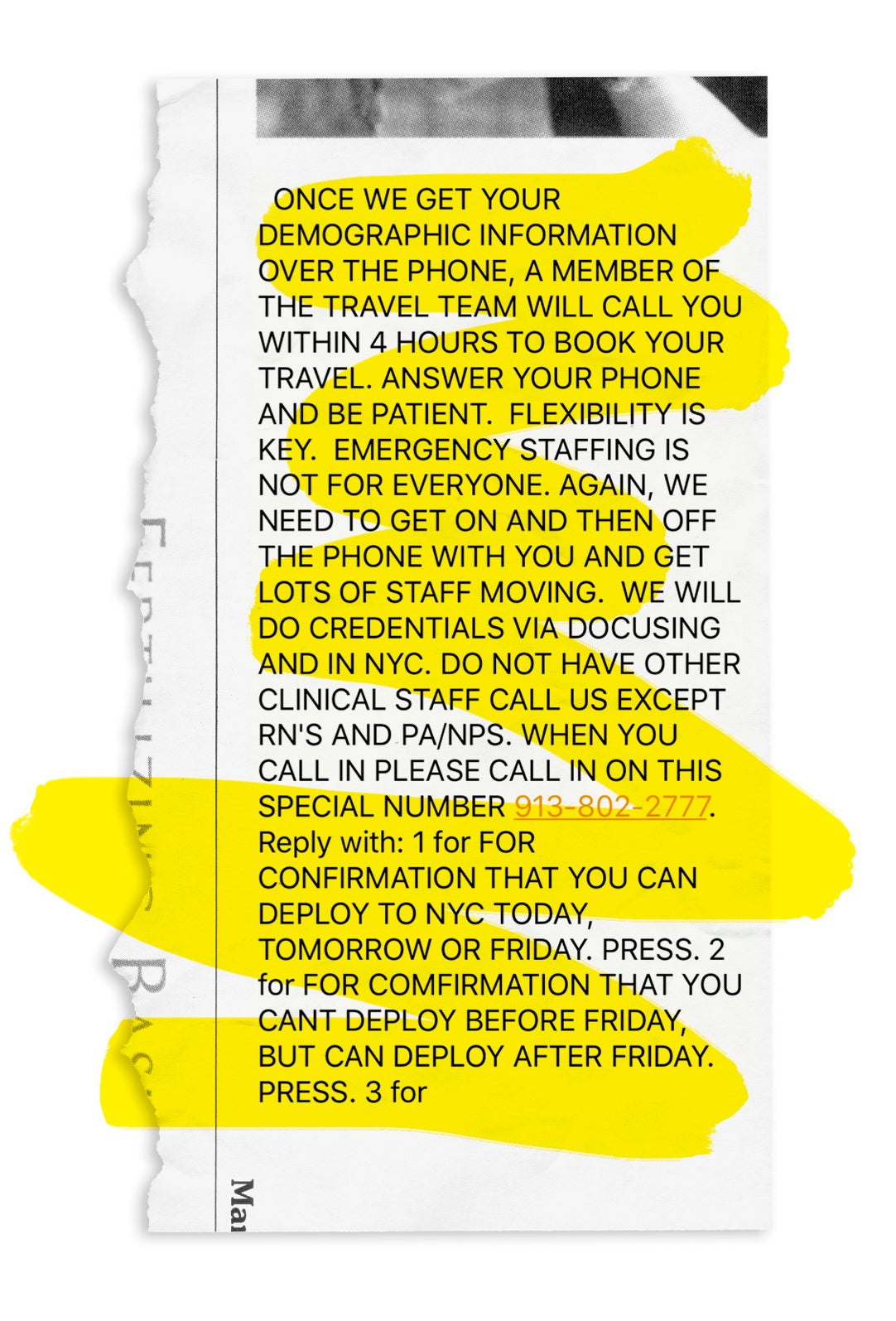
He was staffed full-time at a “much better facility” in California, but Krucial’s proposed payday was enough for him to repeatedly call the agency and endure hours of busy signals just to get an interview, then fly across the country within 36 hours to the epicenter of the virus, without anything in writing. Krucial CEO Brian Cleary admits that although they try to send paperwork over electronically within 24 hours of the initial phone pitch, some eager nurses might get on a plane before that happens. “It depends,” Cleary, a former ER nurse and travel nurse himself, tells us. “We send over 4,000 people, so I can’t say exactly when they land and when they get their DocuSign, but we typically send it within 24 hours.”
Zachary was scared, but he never questioned whether or not to get on that plane. He assumed there would be plenty of nurses waiting through busy signals, ready to take his place if he wavered.
And while 30 grand may seem like a lot for less than a month of labor, compared to the price for his life, it’s a tragically cheap bounty. CDC officials suggest health-care workers account for 11 percent of all coronavirus cases, while the number of deaths remains a mystery, despite President Trump promising he would release the data. National Nurses United, however, says at least 48 of them have died from coronavirus.
48 nurses in the United States have already lost their lives to #COVID19.
That's 48 too many.#ProtectNurses –> No more nurse deaths!https://t.co/spJxbzaBQw
— NationalNursesUnited (@NationalNurses) April 21, 2020
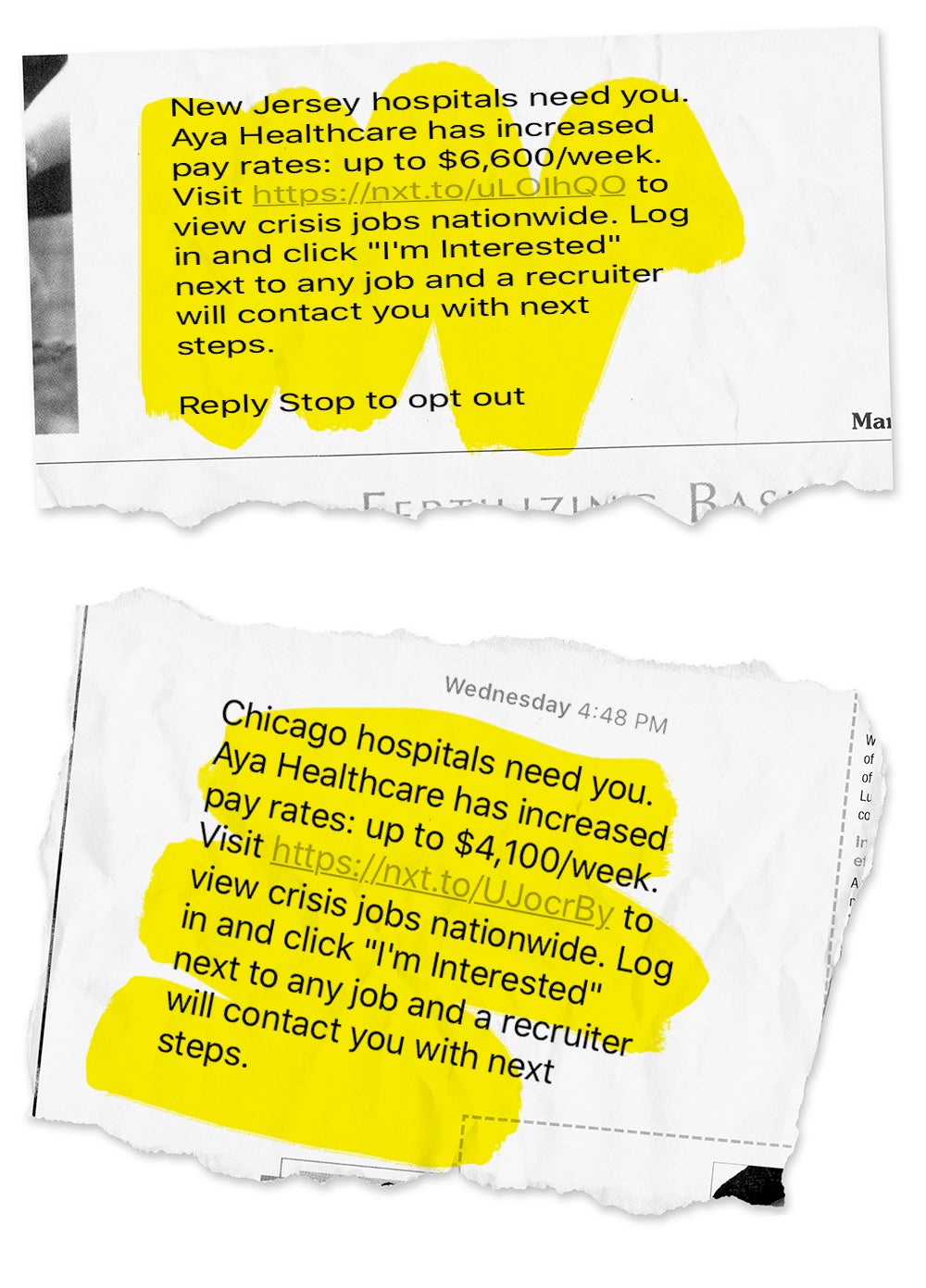
Yet as the death toll rises, so too do recruitment agencies’ rates. Nurses in New Jersey could land $6,600 a week; those in Chicago, $4,100 a week. Zachary’s contract to work 21 days at a hospital in Brooklyn was for $10,000 a week. More generally, Krucial’s 21-day contract nurses get paid $95 per hour for 40 hours a week, time and a half for an additional 44 hours a week, as well as a $76 daily food allowance and a one-time $600 travel stipend. During past deployments like Hurricane Sandy, agencies have offered around $5,000 to $7,000 a week, Cleary estimates. As a point of comparison, nurses who have less than five years experience make $29.62 per hour on average.
“We’ve done hurricanes, border crises, all kinds of events, but nothing compared to this,” Cleary says. “When we were activating for New York, we were rostering roughly 500 nurses in four hours, which is unbelievable.”
Recruitment agencies like Krucial have sprouted up to do the recruiting and hiring for hospitals ever since New Orleans needed extra nurses to help in the ER during Mardi Gras in 1978. Though this was supposed to be a short-term fix, hospitals found great benefit in hiring nurses as independent contractors during national disasters like Hurricane Harvey, the California wildfires and now the COVID-19 crisis, because it’s better for their bottom line. They don’t have to guarantee health benefits or even stable employment to these nurses, whose contracts hospitals can cancel whenever they want.
At their side, travel nursing agencies function as the middleman, brokering these deals and taking their cut from the nurse’s paycheck, which may explain why the median salary for a nurse recruiter is higher than that of the nurses they recruit. “Different companies want to get contracts from that hospital so they get a percentage,” says Shannon, a 27-year-old travel nurse from North Carolina. (Shannon is also a pseudonym; all the names of the nurses quoted throughout have been changed due to their fear of reprisal from agencies.) “That’s how recruiters make money. It’s a whole hustle.”
For the most part, nurses are fine with the system. Travel nursing isn’t for everyone, but particularly for younger nurses who want experience, or those who value pay over benefits, the inherent instability of living contract to contract while bouncing around different cities isn’t a dealbreaker.
The bigger problem is that nurses of all stripes can’t rely on the health-care system or a union to protect them — only 20.4 percent of all nurses belong to unions, typically of the regional variety as there is no overarching national nurses union, and exclusively from permanent salaried positions. The reason why their organizing efforts haven’t been more effective is that many nurses aren’t willing to compromise patient care by picketing. Moreover, when strikes do happen, the highest paid travel nurses, known pejoratively as “scab nurses,” fill in for protesting nurses, weakening their collective leverage as health-care workers overall.
“They call it crossing the line, or the picket out front. The travel nurses have to walk through that, and they do get a lot of hate,” explains Shannon, who worked as a scab nurse two years ago in Vermont at a hospital she wouldn’t disclose. “It’s not violent, but there’s a lot of animosity.”
Picketing nurses are understandably angry about how much scabs make, while they have their pay docked. That said, Shannon claims the hostility is much worse for the permanent nurses who chose to work during the strike because there’s already an existing relationship there, making things personal. To that end, hospitals put a lot of resources into talking nurses out of organizing and breaking up unions.
“The main obstacle to nurses trying to unionize is the union-busting industry, which is very active in health care,” explains Rebecca Givan, professor of labor studies and co-director of the Rutgers Center for Work and Health. When there is a threat of a strike, most hospitals will hire consulting firms to send out mass anti-union emails, distribute anti-union materials in break rooms, hold mandatory anti-union meetings, and of course, threaten nurses engaging in organizing activity by calling security on them.
As such, hospitals end up spending upwards of $11 million to combat strikes, instead of footing the more affordable bill to meet nurses’ demands, despite the fact that multiple studies confirm that accommodating unionizing nurses yields better patient outcomes. “Most health-care employers spend thousands of dollars per employee when nurses attempt to organize a union,” Givan says.
In fairness, it’s difficult to blame travel nurses for taking these positions and doing what they have to do to pay their bills and take care of their families. Shannon, for instance, is a single mom who got into travel nursing when she got divorced. “North Carolina doesn’t allow for legal separation until you’re outside of the home,” she tells us. “So travel nursing allowed me to move out while we figured out our mortgage and custody.” Nevertheless, they, too, are set up to work without a third party that could advocate for benefits, safer working conditions and review the precarious fine print in the crisis contracts, like the one Zachary says he didn’t get to see until he flew across the country.
Throughout his entire three-week deployment, Zachary receives one paid sick day. If he tests positive for coronavirus, however, he will get two weeks paid to quarantine in a hotel, the bill footed by the agency. It’s unclear, though, if Krucial’s health benefits would extend further if he were to suffer complications beyond those two weeks, which many people do; consequently, he pays out-of-pocket for his own health insurance.
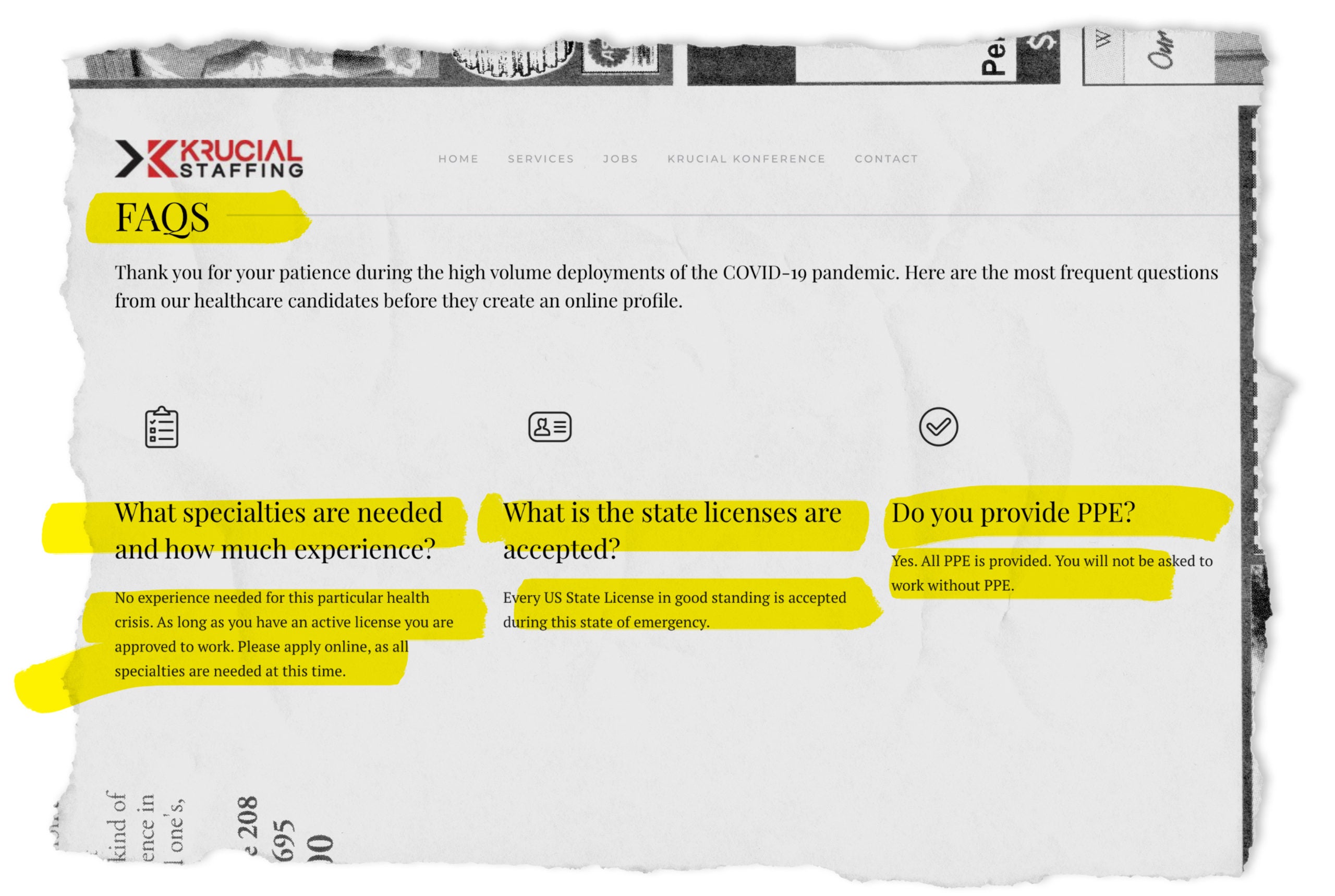
Also, nowhere in the 18 pages of the 21-day crisis contract from Krucial, which was provided anonymously to us, is personal protective equipment, or PPE (masks, gloves and gowns), guaranteed. (It is, however, promised in their job listings.) Instead, it notes that “employees should follow OSHA and their client facility’s policies and procedures” when it comes to protective equipment and gear.
Krucial’s website goes as far as to say “you won’t be asked to work without it,” but Zachary admits that he had to solicit donations independently to get adequate protection. “I went to social media and just told people my situation, and luckily, they donated a bunch of PPE so I can have fresh gear everyday.” (The terms and conditions of the contract does cover jewelry, name tags and even what type of nails nurses are allowed to have — hint: not acrylic.)
Cleary repeatedly claimed that Krucial nurses don’t have to work without PPE, but when we ask why it wasn’t guaranteed in their contracts, he hedges: “We don’t provide PPE; we never have. We’re a staffing agency, so we provide people. That’s pretty standard.”
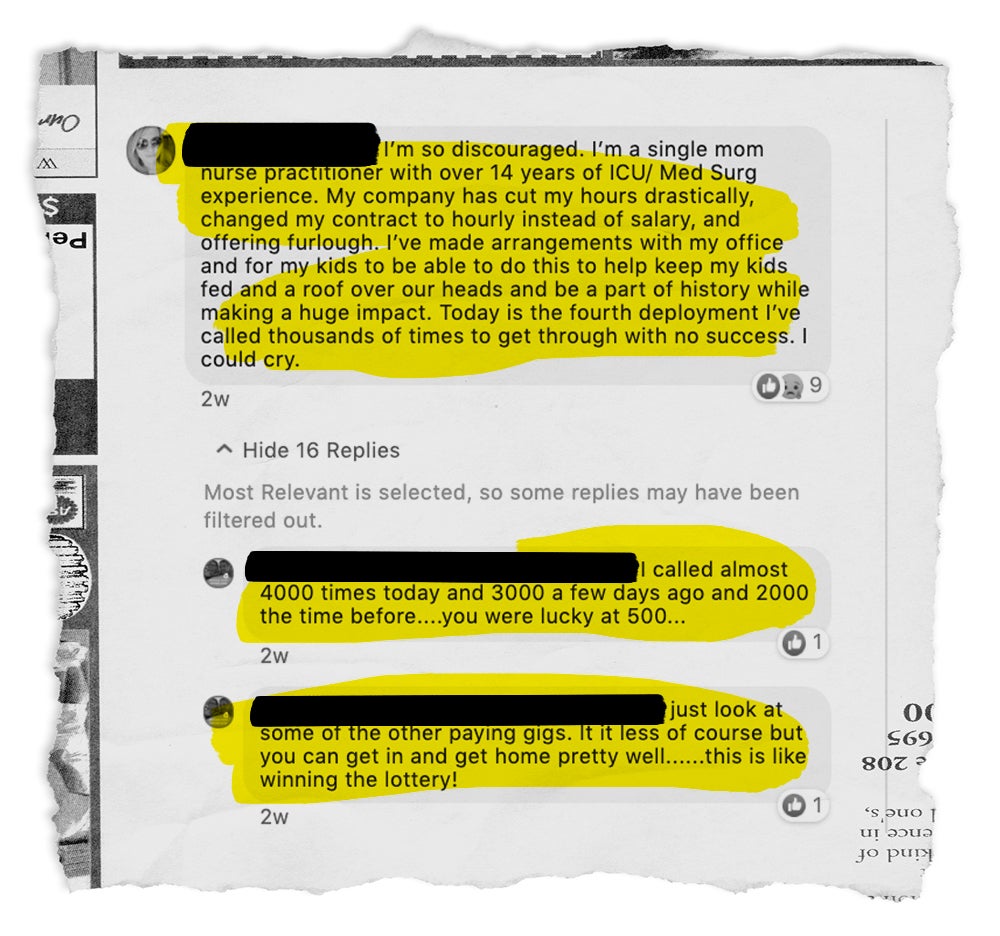
Still, the pay is so competitive, it makes it difficult to negotiate things like PPE, health insurance and sick days. “If you tried to negotiate, I’m sure they’d just decline and there’d be hundreds of nurses in line behind me ready to take my spot,” Zachary says. Krucial’s reservist list and Facebook page are flooded with posts from nurses begging to work, speaking to this cutthroat environment. It’s also worth noting that despite the crush of COVID patients, thousands of nurses in departments like the OR are being laid off because non-essential surgeries and appointments have been put on hold.
“Krucial didn’t have to do any advertising, they sent a mass text to tons of nurses right when everyone was being laid off,” says Gregory Antollino, an attorney representing three nurses who are suing Krucial. “So people couldn’t get through even to apply for a job, and now they’re acting as if ‘everyone wants us, we don’t give a shit if you don’t get PPE, you should just go home.’” Antollino’s lawsuit argues that the recruitment agency has been “profiteering from the crisis, putting nurses’ lives at risk and making promises that its CEO knew he couldn’t keep.”
Cleary dismisses these accusations as hearsay. “I always say 95 percent, but probably closer to 98 percent of people we send are like, ‘When can I go on the next one? This was awesome.’ But there are always a few people who aren’t happy for whatever reason,” he says.
Within the complaint, the plaintiffs (one travel nurse, and two non-travel nurses) allege the company, among other things, lures nurses in with mass texts, phone calls and posts on social media with promises they don’t keep. Krucial “takes in close to double what it pays its workers,” the complaint reads, “[while subjecting] unsuspecting nurses to physical harm by requiring work without proper protective gear [and requiring] them to work outside of their fields of competence.”
In response, Cleary defers to a statement from Krucial’s legal team:
“Krucial Staffing vehemently denies recent claims made in the media related to a lawsuit that has been filed. We would like nothing more than to comment and defend our company from these false allegations, but since this is a legal matter we are unable to do so right now on the advice of counsel.
“We clearly communicate to all our healthcare staff that we do not want them to start any shift if they do not have all the proper protective equipment they need. Krucial Staffing will continue to serve the medical professionals we are so fortunate to work with as we all strive to play a small role in winning this battle against COVID-19.”
Still, Zachary believes he’s got the best nursing gig out there right now, as at least it comes close to compensating him for the dangers he faces. “You have to look out for yourself. The hospital definitely isn’t, and the agency is only going to do the minimum,” he explains. On Day 21, he extended his Krucial contract and declined to speak to us any further, citing that he wanted to “focus on his work.”
“Bigger risks mean bigger rewards,” says Mike, a 32-year-old ICU nurse in West Texas who quit his job and called one of the many recruitment firms who had contacted him about flying to New York. Mike is currently serving a 48-hour per week contract at a New York hospital for $6,000 a week through an agency he didn’t disclose, but says is not Krucial. (There are numerous others such as Faststaff, Nomad Health and Aya.) Before, Mike was making about $2,000 per week. “The risk was always there with COVID, and being an ICU nurse, I was going to have to deal with this at some point in time,” he says. “I figured I might as well be paid for it and social distance from my family at the same time.”
As for what recruiters are looking for, Melissa, a nurse in Minnesota who also traveled to New York, says, “They typically require you to have at least two years experience in your specialty so that you can hit the ground running when you get to your assignment.” But after being recruited on LinkedIn by an agency she doesn’t feel comfortable disclosing, she found the headhunters were only requiring one year, “and stated that it didn’t matter what specialty you have.”
“In the world of nursing, one year is still considered to be extremely novice,” she continues. “I reiterated to everyone I spoke to in this process that I don’t have medical hospital experience. I was told along the way that this wouldn’t be an issue, that they would provide training, and that I’d likely be assigned to a role that used my specialty and skills anyway. This didn’t happen.”
When Melissa arrived at the hospital in New York, she asked her team lead what she and other nurses not trained in this specific setting should do, only to be told, “Well, you’re gonna have to learn really quickly.” “In retrospect, this shouldn’t have been surprising to me,” she says. “They did no employer reference checks, no interviews, nothing. It was basically like, ‘Can you leave on 24 hours notice, and do you have anywhere you refuse to go? Okay, good, you’re hired!’”
Cleary concedes that Melissa’s experience isn’t unique. “I’m sure in a crisis that’s happened, but nurses shouldn’t ever engage in a procedure they’re not comfortable with,” he says. He’s quick to add, however: “A lot of nurses have heroically gone outside of that and done what they had to do.”
Ultimately, Melissa returned to Minnesota before her shift started. Had she stayed, the conditions would have been grim, but still better than they are for staff nurses, who suffer the same risk for less than $30 an hour. “We aren’t getting hazard pay or bonuses,” says Chelsea, an ICU staff nurse just outside of New York City. “I don’t make any more than I ever did before. I’m risking my life by going into these rooms with inadequate PPE. But they won’t pay me for the extra threat, and if I die from this, my family only gets the death benefits that I’d already selected back in November.”
Several months ago, Chelsea spent $180 on hazmat suits, a half-mask respirator, goggles and a face shield in preparation for when her hospital completely runs out. “I’m 100 percent okay with working in a COVID ward, but I will never work without PPE,” she tells us.
“We’re all having to reuse what are supposed to be single-use masks,” adds Ginger, a travel nurse from Georgia who is working with a Krucial competitor and nearing the end of her 21-day contract in New York. “There are essentially no rules, but knowing how deep this connects to our deeply fucked-up and corrupt health-care system, it doesn’t surprise me.”
It might make the public feel good, but these nurses need a lot more than 7 p.m. applause breaks and Facebook commercials calling them heroes. “We feel abandoned by nearly everyone,” Chelsea says. “We’ve had our tires slashed, been yelled at, assaulted and stabbed because we went grocery shopping in scrubs. We’re trying our best to do what we can, but honestly, some days it feels like we’ve been thrown under the bus and run over and left for dead.”
“Don’t worry though,” she adds sarcastically, “we’ll get a pizza party for Nurses Week.”
After putting a lot of thought into her options, then, Shannon has decided it isn’t worth any amount of money to keep working as a nurse during the pandemic because she’s immunosuppressed and has a young son. But after more than five years in travel and permanent positions, it wasn’t an easy decision to make. Like many nurses who want to use their training for the greater good, she never imagined having to think about a different career — and per a recent survey of 1,300 nurses from 400 hospitals in the U.S., this sentiment is quickly becoming a massive problem.
Three out of five nurses responded that they’re “likely to leave their position or specialty as a result of their experience with coronavirus,” and 67 percent of respondents “will either leave their current facility or quit the industry altogether.” These numbers come on the precipice of a nursing shortage that was expected to happen before coronavirus even happened. “The U.S. was already projected to have a shortfall of over 1 million nurses by 2022, due mainly to waves of Baby Boomer-era nurses aging out of the nursing workforce,” explains Darrell Spurlock Jr., the director of the Leadership Center for Nursing Education Research at Widener University in Pennsylvania.
Any fix won’t be cheap. Analysts predict an exodus of nurses due to coronavirus could cost the U.S. an additional $88 billion to $137 billion. “For too long nurses have had to bear the brunt of this health-care system, and now we’re being forced to decide whether or not we want to stay in it at all,” Shannon says. “And I think we’re going to lose a lot of good people.”
“It’s all a big money-making scam,” Chelsea adds. “Profits mean more to hospital CEOs than patients or the staff, and nothing will change until that focus reverses, because it can’t be both.” In the meantime, she says, “It’s created a horrible work environment that grinds nurses down like grain on a millstone. It’s soul-sucking and demoralizing.”
There are some steps lawmakers could take to prevent a nursing shortage. “Many hospitals have cut down on the number of ancillary staff available such as patient care techs and secretaries. This means that nurses often end up doing three jobs at once,” Chelsea says. So to start, “we need safe [nurse-to-patient] staffing ratios, adequate and safe PPE, hazard pay for taking care of COVID-19 patients and a student loan forgiveness grant.”
After that, she’d like to see some accountability. The same goes for Ginger, who hopes that, if anything, that’s the silver lining in the hell that she and her fellow nurses are currently suffering through. “I feel like this might be the Achilles’ heel of our current state of health care, and that there may be huge shifts in the future — hopefully, in the altruistic direction.”

Lauren Vinopal
Lauren Vinopal is a writer and stand-up comedian based out of New York City, who writes mostly about health, science and men. She is the host of the Mid Riff Comedy Show in Brooklyn, a frequent podcast guest all over, and lives the life of a teen who looks like they haven’t slept in years.

Quinn Myers
Quinn Myers is a staff writer at MEL. He reports on internet culture, technology, health, masculinity and the communities that flourish within.